


04.04.22
By Julius Few, MD; Michael Lee, MD; Alec Semersky; Emily Mariscal, LE; and Ginny Vachon, PhD
This article originally appeared in the Aesthetic Surgery Journal.
Retinol is known to reduce the appearance of fine lines and wrinkles, but is associated with irritating effects. Cannabidiol (CBD) acts to reduce oxidative stress and inflammation, mitigating irritation from retinol, and further improving the skin’s appearance through independent anti-aging mechanisms.
Skin aging is influenced by a number of factors, including extrinsic factors like exposure to UV light, poor diet, or pollutants, and intrinsic factors such as collagen and elastin loss over time.1 Within the skin, intrinsic aging is due, in part, to the decreased capacity of keratinocytes, fibroblasts, and melanocytes to proliferate, and the degeneration of the fibrous extracellular matrix, while 80% of extrinsic aging can be attributed to UV radiation.2-4 Interestingly, for both intrinsic and extrinsic aging, reactive oxygen species (ROS) and associated oxidative stress can accelerate these processes in the skin through multiple mechanisms and contribute to dyspigmentation, reduced barrier function, laxity, and uneven texture.1-5 In addition, ROS are associated with inflammation, which can further negatively impact the skin’s appearance.5,6
In clinical practice, one of the few topical treatments for which there is strong clinical evidence of efficacy for reducing the signs of aging is retinol.7 The anti-aging effects of retinol are manifested by promoting proliferation of keratinocytes, strengthening the epidermis, and increasing collagen. However, retinol may indirectly decrease the antioxidative effects of the skin, leaving it prone to damage from ROS.8-10 Furthermore, skin reactions such as redness, drying, peeling, or burning associated with retinol treatment can lead to inconsistent use or discontinuation by patients.
In the current study, purified, water-soluble CBD was evaluated with 0.2% retinol as a combination product (CR-Topical, Aforé, Chicago IL). By combining these agents, CR-Topical face cream was designed to combat both the intrinsic and extrinsic factors involved in skin aging by increasing skin turnover while protecting the skin through antioxidative and anti-inflammatory mechanisms, such that both efficacy and tolerability is improved.
In the current pilot study, due to the novelty of the combination and the need to characterize the impact of these treatments on the skin, a more granular approach was taken to measuring outcomes. Typically, aesthetic conditions are measured using validated and non-validated scales (e.g., FACE-Q, GAIS) using static photos taken from multiple angles.11,12 Subject satisfaction questionnaires may also be used to gauge perceptions of efficacy, satisfaction, and overall impressions. However, these scales are limited in their ability to detect specific changes to features such as skin quality. Therefore, the nine-domain Global Ranking Scale (GRS) and four-domain Skin Quality assessment was applied.13 The GRS is unique in that it is used as a collaborative tool by the physician with the patient, and therefore additional methods, described below, were used to confirm observations, including: blinded review and ordering of before and after images by a board-certified plastic surgeon, and inclusion of patient survey questions, which were completed independently, that overlap with GRS skin quality domains to confirm outcomes.
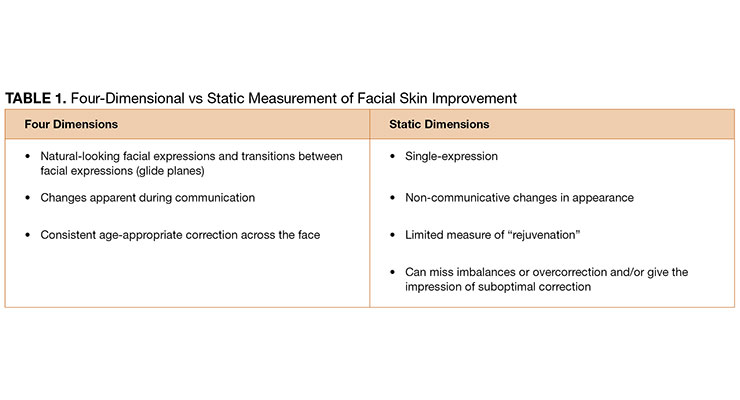
In addition to the capture of static images, this study evaluated patients using video of a series of facial expressions as an exploratory endpoint. Even the best before and after static images represent an incomplete picture of treatment efficacy. Moreover, optimal static correction can result in unnatural mimetic movement, overfilling, and/or inadequate or imbalanced correction. Compared with static images, dynamic videos are better able to capture global improvement across four dimensions, encompassing glide plane movement and multiple facial expressions (Table 1). The use of videos in this study was exploratory in nature and represents the first time that this four-dimensional beauty (4D Beauty, Aforé, LLC, Chicago IL) assessment has been used in a clinical study. So much of how patients perceive themselves and are perceived by others is embedded in expressions, and even qualities like facial positioning and openness can be appreciated with video. This type of assessment is in its infancy, and development will likely involve extensive multidisciplinary research and development of novel measures, as well as protocols for video capture, however, its inclusion here paves the way for further development. In this pilot study, the use of 4D Beauty assessment is detailed, but is not part of the formal evaluation of efficacy. However, this work paves the way for use in clinical practice and study.13,14
Subjects who had botulinum toxin or filler within 3 months of study enrollment were excluded. Additionally, subjects who used topical, inhaled, or ingested cannabis and/or hemp-derived products including CBD or tetrahydrocannabinol within 30 days of the study start date or during the study period were excluded. Further key exclusionary characteristics included facial rejuvenation procedures (e.g., chemical peels, microneedling, microdermabrasion, etc.); pregnancy; advanced or poorly controlled diabetes; current smoker or history of heavy smoking; the use of anti-inflammatory topical products during the study period; or regular continuous use of systemic or topical corticosteroids on the area to be treated.
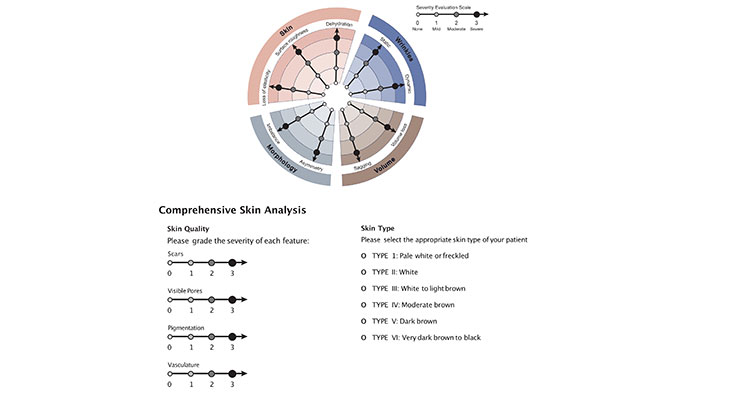
The primary efficacy endpoint consisted of clinical evaluations of the face based on comparison of GRS scores at each time point, compared to baseline, as well as qualitative comparison of standardized before and after photographs on days 1, 21, and 42. During visits on day 1 (baseline), 21, and 42, standardized photographs of the treatment areas were taken and global skin appearance was assessed using the GRS with Comprehensive Skin Analysis by joint evaluation of severity by the lead investigator and the subject (Figure 1).13
Note, the investigator and subject were blinded to their original assessment scores at the time of evaluation. Each of the scale’s 13 domains, including loss of elasticity, surface roughness, dehydration, static and dynamic wrinkles, volume loss, sagging, asymmetry, imbalance, scar presence, visible pores, pigmentation, and vasculature, were graded from 0-3 (0, none; 1, mild; 2, moderate; 3, severe), and mean scores at baseline and at 42 days were calculated for each domain and compared.13 Paired mean difference with each subject used as their own control, and lower and upper 95% confidence intervals for each domain was calculated. Due to the small number of subjects and the use of a 4-point scale across numerous domains, paired t-tests with p-values are less informative (p-values calculated using a paired two-tailed t-test were significant for all measures assessed), and are not presented here.
Because the GRS is intended to be used as a collaborative tool by the physician with the patient, it is not conducive to blinded review. Instead, a blinded reviewer was asked to order the static baseline and 42-day images as before and after, and percent agreement with whether the actual photograph was taken at baseline or day 42 was calculated. In addition, questions overlapping with GRS skin quality domains were included in the subject questionnaire to confirm outcomes. These questionnaires were completed by subjects independently, following completion of the GRS.
Secondary efficacy endpoints included subject observations from satisfaction questionnaires regarding major cutaneous changes such as smoothness, irritation, pruritus, burning, and erythema. Exploratory endpoints included the use of 4D assessment as an assessment tool for qualitative measure of dynamic and animation-related patient features. On days 21 and 42, daily subject diaries were reviewed for compliance and tolerability, and subjects completed an 8-question satisfaction survey. Filmed video evaluations occurred on days 1 and 42 for 4D assessment.
Safety was monitored by the investigator through application site assessment during each follow-up visit (days 1, 21, and 42). Because of the established propensity for retinol to cause irritation, an additional, virtual safety assessment of the application site occurred on day 3. At each follow-up visit, study medication tubes were weighed for compliance. This study was IRB approved (Advarra IRB, Columbia, MD) and adhered to the Good Clinical Practice and standards set forth in the World Medical Association’s Declaration of Helsinki. Written consent was provided, by which the patients agreed to the use and analysis of their data.
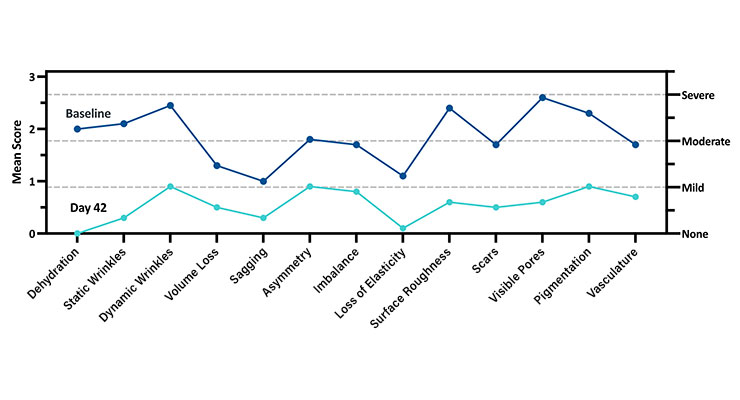
At 42 days, GRS with Comprehensive Skin Analysis score improvement was observed from baseline to day 42 across all 13 domains, including domains for which improvement was unexpected (e.g., sagging). While improvement was consistent, some areas improved more than others, generally those most consistent with a topical treatment (Figure 2). Among subjects, the highest mean scores at baseline were visible pores (2.6), dynamic wrinkles (2.5), surface roughness (2.4), pigmentation (2.3), and static wrinkles (2.1); Higher mean scores correlate to worse skin quality [0, none; 1, mild; 2, moderate; 3, severe]).
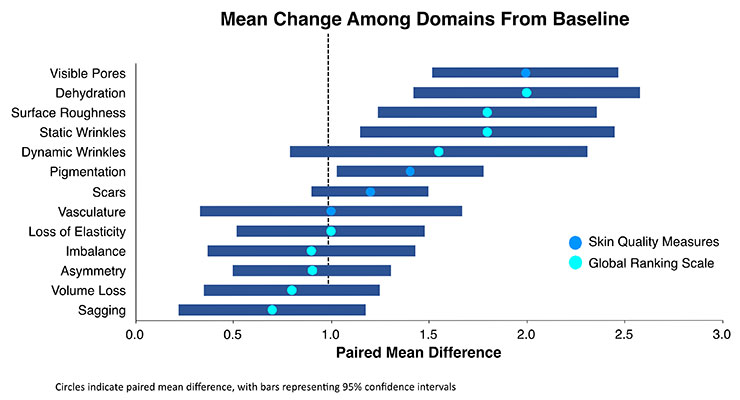
When assessing the relative degree of improvement for each domain, those with ≥ 1-point improvement from day 0 to day 42 were found to be consistent with topical treatments (Figure 3, black dotted line). While statistically significant changes were observed for each domain, including both the GRS and skin quality measures, the areas of greatest change were visible pores (2.0-point change; 95% CI, 1.5-2.5), dehydration (2.0-point change; 95% CI, 1.4-2.6), surface roughness (1.8-point change; 95% CI, 1.2-2.4) static wrinkles (1.8-point change; 95% CI, 1.1-2.5), and dynamic wrinkles (1.6-point change; 95% CI, 0.8-2.3). Notably, while the greatest possible score change is 3, not all subjects began with “severe” skin quality, making a 3-point change impossible. However, a two-point change represents a change from “severe” to “mild” or “moderate” to “none,” both of which represent very impactful improvements.
Each subject who reported severe static wrinkles, dynamic wrinkles, surface roughness, scars, visible pores or vasculature at baseline reported at least “mild” severity for these domains at study completion. Moreover, all subjects with “severe” dehydration reported “none” at the end of the study. The blinded reviewer correctly ordered before and after images for 80% of the subjects.
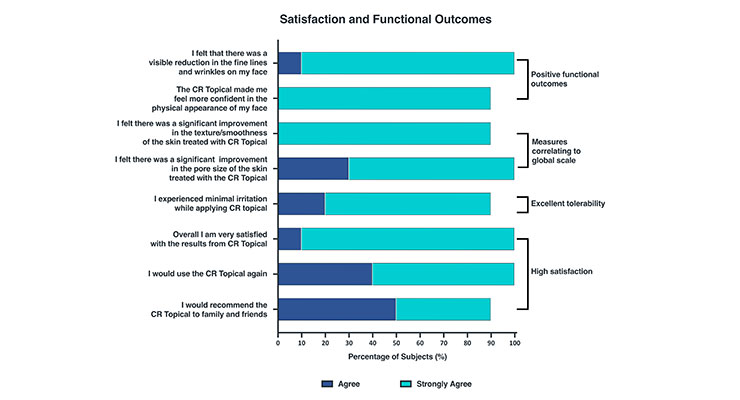
Satisfaction and functional outcomes assessed using subject questionnaires completed on days 21 and 42 revealed that at day 42, 90% of subjects either agreed (50%) or strongly agreed (40%) that they experienced visible reduction of facial fine lines and wrinkles (Figure 4). Overall, 100% of subjects felt that CR-Topical made them more confident in the physical appearance of their face. In agreement with GRS outcomes, subjects strongly agreed that the use of CR-Topical significantly improved the texture/smoothness (90%) and pore size (70%) of the skin, outcomes consistent with those measured with the GRS. Subjects either agreed or strongly agreed (30% vs 70%, respectively) with the statement that they experienced minimal irritation for the duration of the study, demonstrating the excellent tolerability of CR-Topical. Furthermore, 90% of subjects strongly agreed that they were very satisfied with the product, with 90% expressing both their willingness to use CR-Topical again and recommend the cream to family and friends.
Representative patient images illustrate improvement across a range of GRS domains (Figure 5). Changes in skin quality are apparent in before and after images and show a close-up view of patients so that changes in skin quality can be appreciated.
Although research on CBD oil as a topical agent is still emerging, supplementary use has been shown to decrease inflammation and improve therapeutic outcomes for severe inflammatory skin diseases, supporting this potential role.16-18 Anecdotally, the improvements observed for the combination of retinol and water-soluble CBD are better than for either product alone, suggesting an additive, or potentially synergistic benefit. Larger controlled studies will need to be carried out in order to understand the relative effects of CR-Topical and retinol, and to define any synergistic activity for the two ingredients. Importantly in these studies, a larger number of patients should be followed for an extended period of time to best understand the impact of treatment.
When considering the potential for synergistic activity, the mechanism of action for both retinol and CBD is informative. Through the combined effects of promoting cell proliferation and reducing oxidative stress, these agents may work synergistically to combat both the extrinsic and intrinsic causes of aging. While the mechanism of action of CBD in the skin has yet to be fully elucidated, its antioxidant and anti-inflammatory activities are well recognized, and can be partially attributed to its activation of Nrf2-target activation genes, including HMOX1, which plays crucial roles in modulating inflammation, apoptosis, and oxidative stress.19
Importantly, CBD-induced activation of HMOX1 expression occurs through a Nrf2-independent mechanism.19 Because retinol suppresses expression of Nrf2-target antioxidative genes, the addition of CBD oil can potentially restore antioxidative effects inhibited by retinol while allowing for retention of skin strengthening properties.8,10,18 This activity of CBD is in addition to independent mechanisms, including modulation of the human endocannabinoid system (ECS), which is linked to anti-aging effects through its role in maintaining skin homeostasis and barrier function, antioxidant and anti-inflammatory activity, as well as optimal sebum production.18-20
For retinol, independent effects are manifested through promoting keratinocyte proliferation, strengthening of the epidermis and increasing collagen (through protection of existing collagen and stimulation of neocollagenesis) in the skin.8,9 Importantly, the combination of CBD and retinol appears to reduce skin irritation often observed with retinol alone. Notably, 100% of subjects who reported “severe” dehydration at baseline reported “none” at the conclusion of the study, indicating that CBD may combat the irritation characteristic of retinol topicals, providing considerable benefit to subject tolerability and indirect improvement in efficacy due to increasing the likelihood of adherence. Importantly, the CBD used in this study is water soluble. Most often, CBD is administered dissolved in oil, commonly coconut oil or medium-chain triglyceride (MCT) oil. The absence of oils in this formulation that could potentially clog pores or otherwise irritate skin is also an important contributor.
While improvement across all 13 domains for all subjects suggests a global effect of CR-Topical, improvements in areas such as sagging or asymmetry may signal some variability in day-to-day perceptions, some level of bias that stems from the investigator and the subject completing the assessment together, or incomplete ability of the subject to differentiate entirely between the contributions of individual domains to overall global improvement. In future studies, placebo control and blinding both the subject and evaluating investigator will shed light on this topic. Additionally, when interpreting results, it is important to consider that the rating scale ranged from 0 to 3. Therefore, seemingly modest changes (e.g., “severe” at 3 to “mild” at 1) do indeed reflect a significant improvement. Because of the granular nature of the GRS scale, it is possible that future studies could also evaluate combination treatment with other products or modalities versus monotherapy, further characterizing the effects of distinct interventions on global outcome when used together.
As skin treatments continue to emerge and become increasingly multi-modal in nature, it is essential to better understand the specific effects that different treatments have on the skin. While historical measurements for skin treatment efficacy have relied on static imagery, this methodology cannot capture the movement of glide planes and facial expressions, and it is how our faces move during communication that most informs perceptions of beauty. Capturing movements of the face with short videos more accurately reflects what is observed in day-to-day life as opposed to static imagery, and provides a real-world context for evaluating the most relevant effects of treatment. This novel and dynamic 4D assessment may prevent overcorrection or unnatural looking results by encouraging consideration of youthful dynamics in expression as well as facial proportion.21 Further, 4D assessment can be used in conjunction with new or existing scales and opens the door for incorporation of new measures rating naturalness of outcomes, projection or correction across multiple facial expressions, apparent confidence, openness, or other characteristics that are not traditionally thought of as study outcomes. Moreover, subjects can use the videos to better evaluate their overall satisfaction and experience by observing their facial movements before and after treatment. Like the GRS, 4D assessment can be used as a tool for patient education, treatment planning, and encouraging pursuit of natural-looking results. The exploratory assessment using 4D dynamic imagery in this study revealed that video documentation and 4D beauty is an important element of a comprehensive efficacy profile for any product or device and paved the way for video and dynamic assessments as measures of treatment effect.
Shortcomings of this study include the small sample size and short duration of follow-up time. A larger cohort and increased length of the study could lead to more robust results, especially if the design includes a control group or is a split-face study. Future studies will compare the efficacy of CR-Topical with retinol alone.
When used in combination, water-soluble CBD and retinol offer significant improvements in skin quality, as well as in static and dynamic lines, with minimal irritation. Synergistic activity of CBD and retinol may explain this high level of efficacy. Additionally, a more granular assessment of aesthetic outcomes is long overdue and should be incorporated into future clinical studies evaluating topical skin treatments. Dynamic, 4D beauty assessment is a newly emerging mode of evaluation that could be fully developed and applied to better capture the effects of treatment.
References
1. Zhang S, Duan E. Fighting against skin aging: the way from bench to bedside. Cell Transplant. 2018;27(5):729-738. doi:10.1177/0963689717725755
2. Dimri GP, Lee X, Basile G, et al. A biomarker that identifies senescent human cells in culture and in aging skin in vivo. Proc Natl Acad Sci U S A. 1995;92(20):9363-9367. doi:10.1073/pnas.92.20.9363
3. Kohl E, Steinbauer J, Landthaler M, Szeimies RM. Skin ageing. J Eur Acad Dermatol Venereol. 2011;25(8):873-884. doi:10.1111/j.1468-3083.2010.03963.x
4. Friedman O. Changes associated with the aging face. Facial Plast Surg Clin North Am. 2005;13(3):371-380. doi:10.1016/j.fsc.2005.04.004
5. Rinnerthaler M, Bischof J, Streubel MK, et al. Oxidative stress in aging human skin. Biomolecules. 2015;5(2):545-589. doi:10.3390/biom5020545
6. Tsuchida K, Kobayashi M. Oxidative stress in human facial skin observed by ultraweak photon emission imaging and its correlation with biophysical properties of skin. Sci Rep. 2020;10(1):9626. doi:10.1038/s41598-020-66723-1
7. Mukherjee S, Date A, Patravale V, et al. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging. 2006;1(4):327-348. doi:10.2147/ciia.2006.1.4.327
8. Zasada M, Budzisz E. Retinoids: active molecules influencing skin structure formation in cosmetic and dermatological treatments. Postepy Dermatol Alergol. 2019;36(4):392-397. doi:10.5114/ada.2019.87443
9. Hubbard BA, Unger JG, Rohrich RJ. Reversal of skin aging with topical retinoids. Plast Reconstr Surg. 2014;133(4):481e-490e. doi:10.1097/PRS.0000000000000043
10. Wang H, Liu K, Geng M, et al. RXRα inhibits the NRF2-ARE signaling pathway through a direct interaction with the Neh7 domain of NRF2. Cancer Res. 2013;73(10):3097-3108. doi:10.1158/0008-5472.CAN-12-3386
11. Klassen AF, Cano SJ, Schwitzer JA, Scott AM, Pusic AL. FACE-Q scales for health-related quality of life, early life impact, satisfaction with outcomes, and decision to have treatment: development and validation. Plast Reconstr Surg. 2015;135(2):375-386. doi:10.1097/PRS.0000000000000895
12. Narins RS, Brandt F, Leyden J, Lorenc ZP, Rubin M, Smith S. A randomized, double-blind, multicenter comparison of the efficacy and tolerability of Restylane versus Zyplast for the correction of nasolabial folds. Dermatol Surg. 2003;29(6):588-595. doi:10.1046/j.1524-4725.2003.29150.x
13. Jain R, Huang P, Ferraz RM. A new tool to improve delivery of patient-engaged care and satisfaction in facial treatments: the Aesthetic Global Ranking Scale. J Cosmet Dermatol. 2017;16(1):132-143. doi:10.1111/jocd.12297
14. Cartier H, Hedén P, Delmar H, et al. Repeated full-face aesthetic combination treatment with abobotulinumtoxinA, hyaluronic acid filler, and skin-boosting hyaluronic acid after monotherapy with abobotulinumtoxinA or hyaluronic acid filler. Dermatol Surg. 2020;46(4):475-482. doi:10.1097/DSS.0000000000002165
15. Kim BH, Lee YS, Kang KS. The mechanism of retinol-induced irritation and its application to anti-irritant development. Toxicol Lett. 2003;146(1):65-73. doi:10.1016/j.toxlet.2003.09.001
16. Sholler DJ, Schoene L, Spindle TR. Therapeutic efficacy of cannabidiol (CBD): a review of the evidence from clinical trials and human laboratory studies. Curr Addict Rep. 2020;7(3):405-412. doi:10.1007/s40429-020-00326-8
17. Palmieri B, Laurino C, Vadalà M. A therapeutic effect of cbd-enriched ointment in inflammatory skin diseases and cutaneous scars. Clin Ter. 2019;170(2):e93-e99. doi:10.7417/CT.2019.2116
18. Oláh A, Tóth BI, Borbíró I, et al. Cannabidiol exerts sebostatic and antiinflammatory effects on human sebocytes. J Clin Invest. 2014;124(9):3713-3724. doi:10.1172/JCI64628
19. Casares L, García V, Garrido-Rodríguez M, et al. Cannabidiol induces antioxidant pathways in keratinocytes by targeting BACH1. Redox Biol. 2020;28:101321. doi:10.1016/j.redox.2019.101321
20. Baswan SM, Klosner AE, Glynn K, et al. Therapeutic potential of cannabidiol (CBD) for skin health and disorders. Clin Cosmet Investig Dermatol. 2020;13:927-942. doi:10.2147/CCID.S286411
21. Few JW, Pintas S, Smith JR, Vachon G. Nonsurgical Tissue Repositioning: Analysis of Long-Term Results and Patient Satisfaction From 100 Absorbable Suture Suspension Cases. Aesthet Surg J Open Forum. 2019;2(1):ojz029. doi:10.1093/asjof/ojz029
This article originally appeared in the Aesthetic Surgery Journal.
Retinol is known to reduce the appearance of fine lines and wrinkles, but is associated with irritating effects. Cannabidiol (CBD) acts to reduce oxidative stress and inflammation, mitigating irritation from retinol, and further improving the skin’s appearance through independent anti-aging mechanisms.
Skin aging is influenced by a number of factors, including extrinsic factors like exposure to UV light, poor diet, or pollutants, and intrinsic factors such as collagen and elastin loss over time.1 Within the skin, intrinsic aging is due, in part, to the decreased capacity of keratinocytes, fibroblasts, and melanocytes to proliferate, and the degeneration of the fibrous extracellular matrix, while 80% of extrinsic aging can be attributed to UV radiation.2-4 Interestingly, for both intrinsic and extrinsic aging, reactive oxygen species (ROS) and associated oxidative stress can accelerate these processes in the skin through multiple mechanisms and contribute to dyspigmentation, reduced barrier function, laxity, and uneven texture.1-5 In addition, ROS are associated with inflammation, which can further negatively impact the skin’s appearance.5,6
In clinical practice, one of the few topical treatments for which there is strong clinical evidence of efficacy for reducing the signs of aging is retinol.7 The anti-aging effects of retinol are manifested by promoting proliferation of keratinocytes, strengthening the epidermis, and increasing collagen. However, retinol may indirectly decrease the antioxidative effects of the skin, leaving it prone to damage from ROS.8-10 Furthermore, skin reactions such as redness, drying, peeling, or burning associated with retinol treatment can lead to inconsistent use or discontinuation by patients.
In the current study, purified, water-soluble CBD was evaluated with 0.2% retinol as a combination product (CR-Topical, Aforé, Chicago IL). By combining these agents, CR-Topical face cream was designed to combat both the intrinsic and extrinsic factors involved in skin aging by increasing skin turnover while protecting the skin through antioxidative and anti-inflammatory mechanisms, such that both efficacy and tolerability is improved.
In the current pilot study, due to the novelty of the combination and the need to characterize the impact of these treatments on the skin, a more granular approach was taken to measuring outcomes. Typically, aesthetic conditions are measured using validated and non-validated scales (e.g., FACE-Q, GAIS) using static photos taken from multiple angles.11,12 Subject satisfaction questionnaires may also be used to gauge perceptions of efficacy, satisfaction, and overall impressions. However, these scales are limited in their ability to detect specific changes to features such as skin quality. Therefore, the nine-domain Global Ranking Scale (GRS) and four-domain Skin Quality assessment was applied.13 The GRS is unique in that it is used as a collaborative tool by the physician with the patient, and therefore additional methods, described below, were used to confirm observations, including: blinded review and ordering of before and after images by a board-certified plastic surgeon, and inclusion of patient survey questions, which were completed independently, that overlap with GRS skin quality domains to confirm outcomes.
In addition to the capture of static images, this study evaluated patients using video of a series of facial expressions as an exploratory endpoint. Even the best before and after static images represent an incomplete picture of treatment efficacy. Moreover, optimal static correction can result in unnatural mimetic movement, overfilling, and/or inadequate or imbalanced correction. Compared with static images, dynamic videos are better able to capture global improvement across four dimensions, encompassing glide plane movement and multiple facial expressions (Table 1). The use of videos in this study was exploratory in nature and represents the first time that this four-dimensional beauty (4D Beauty, Aforé, LLC, Chicago IL) assessment has been used in a clinical study. So much of how patients perceive themselves and are perceived by others is embedded in expressions, and even qualities like facial positioning and openness can be appreciated with video. This type of assessment is in its infancy, and development will likely involve extensive multidisciplinary research and development of novel measures, as well as protocols for video capture, however, its inclusion here paves the way for further development. In this pilot study, the use of 4D Beauty assessment is detailed, but is not part of the formal evaluation of efficacy. However, this work paves the way for use in clinical practice and study.13,14
Methods of Pilot Study
This single-center pilot study evaluated the efficacy, safety, and tolerability of CR-Topical (300 mg of purified, medical grade, water-soluble CBD; 0.2% retinol; proprietary botanicals and stabilizing agents) applied once daily to the facial skin. The study enrolled 10 healthy female subjects between 20 and 53 years of age who presented with any combination of the following on the facial skin: visible pores, dehydration, roughness, static or dynamic wrinkles, skin laxity, and/or facial fine lines. Subjects were informed of the potential for exposure to CBD, and were blinded as to whether they were receiving active treatment or placebo. Each subject was provided with a tube of CR-Topical labeled “A” by the manufacturer and instructed to apply 2 pumps (0.3 ml) of CR-Topical to their entire facial skin in the evening before bed after using a mild facial cleanser. After enrollment, subjects immediately began treatment and continued the regimen for 42 days (6 weeks) until study completion. For the duration of the study, subjects were asked to fill out a daily log detailing any changes to their skin appearance and any side effects they experienced. Subjects served as their own control.Subjects who had botulinum toxin or filler within 3 months of study enrollment were excluded. Additionally, subjects who used topical, inhaled, or ingested cannabis and/or hemp-derived products including CBD or tetrahydrocannabinol within 30 days of the study start date or during the study period were excluded. Further key exclusionary characteristics included facial rejuvenation procedures (e.g., chemical peels, microneedling, microdermabrasion, etc.); pregnancy; advanced or poorly controlled diabetes; current smoker or history of heavy smoking; the use of anti-inflammatory topical products during the study period; or regular continuous use of systemic or topical corticosteroids on the area to be treated.
The primary efficacy endpoint consisted of clinical evaluations of the face based on comparison of GRS scores at each time point, compared to baseline, as well as qualitative comparison of standardized before and after photographs on days 1, 21, and 42. During visits on day 1 (baseline), 21, and 42, standardized photographs of the treatment areas were taken and global skin appearance was assessed using the GRS with Comprehensive Skin Analysis by joint evaluation of severity by the lead investigator and the subject (Figure 1).13
Note, the investigator and subject were blinded to their original assessment scores at the time of evaluation. Each of the scale’s 13 domains, including loss of elasticity, surface roughness, dehydration, static and dynamic wrinkles, volume loss, sagging, asymmetry, imbalance, scar presence, visible pores, pigmentation, and vasculature, were graded from 0-3 (0, none; 1, mild; 2, moderate; 3, severe), and mean scores at baseline and at 42 days were calculated for each domain and compared.13 Paired mean difference with each subject used as their own control, and lower and upper 95% confidence intervals for each domain was calculated. Due to the small number of subjects and the use of a 4-point scale across numerous domains, paired t-tests with p-values are less informative (p-values calculated using a paired two-tailed t-test were significant for all measures assessed), and are not presented here.
Because the GRS is intended to be used as a collaborative tool by the physician with the patient, it is not conducive to blinded review. Instead, a blinded reviewer was asked to order the static baseline and 42-day images as before and after, and percent agreement with whether the actual photograph was taken at baseline or day 42 was calculated. In addition, questions overlapping with GRS skin quality domains were included in the subject questionnaire to confirm outcomes. These questionnaires were completed by subjects independently, following completion of the GRS.
Secondary efficacy endpoints included subject observations from satisfaction questionnaires regarding major cutaneous changes such as smoothness, irritation, pruritus, burning, and erythema. Exploratory endpoints included the use of 4D assessment as an assessment tool for qualitative measure of dynamic and animation-related patient features. On days 21 and 42, daily subject diaries were reviewed for compliance and tolerability, and subjects completed an 8-question satisfaction survey. Filmed video evaluations occurred on days 1 and 42 for 4D assessment.
Safety was monitored by the investigator through application site assessment during each follow-up visit (days 1, 21, and 42). Because of the established propensity for retinol to cause irritation, an additional, virtual safety assessment of the application site occurred on day 3. At each follow-up visit, study medication tubes were weighed for compliance. This study was IRB approved (Advarra IRB, Columbia, MD) and adhered to the Good Clinical Practice and standards set forth in the World Medical Association’s Declaration of Helsinki. Written consent was provided, by which the patients agreed to the use and analysis of their data.
Results of Study
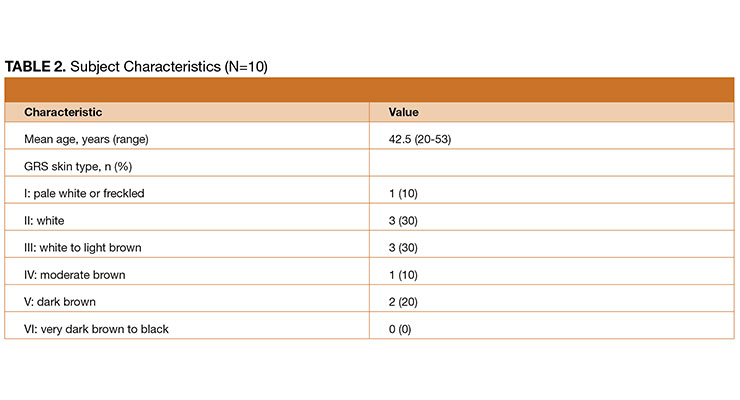
Ten subjects were enrolled in this pilot study, with a median age of 42.5 (Table 2). A greater proportion of subjects had either white (30%) or white to light brown (30%) skin compared with other skin types, as determined using the GRS scale.13 All 10 subjects reported using CR-Topical once daily at night before bed for 42 days and product weight was consistent with the high level of compliance reported. No subjects were lost to follow up.At 42 days, GRS with Comprehensive Skin Analysis score improvement was observed from baseline to day 42 across all 13 domains, including domains for which improvement was unexpected (e.g., sagging). While improvement was consistent, some areas improved more than others, generally those most consistent with a topical treatment (Figure 2). Among subjects, the highest mean scores at baseline were visible pores (2.6), dynamic wrinkles (2.5), surface roughness (2.4), pigmentation (2.3), and static wrinkles (2.1); Higher mean scores correlate to worse skin quality [0, none; 1, mild; 2, moderate; 3, severe]).
When assessing the relative degree of improvement for each domain, those with ≥ 1-point improvement from day 0 to day 42 were found to be consistent with topical treatments (Figure 3, black dotted line). While statistically significant changes were observed for each domain, including both the GRS and skin quality measures, the areas of greatest change were visible pores (2.0-point change; 95% CI, 1.5-2.5), dehydration (2.0-point change; 95% CI, 1.4-2.6), surface roughness (1.8-point change; 95% CI, 1.2-2.4) static wrinkles (1.8-point change; 95% CI, 1.1-2.5), and dynamic wrinkles (1.6-point change; 95% CI, 0.8-2.3). Notably, while the greatest possible score change is 3, not all subjects began with “severe” skin quality, making a 3-point change impossible. However, a two-point change represents a change from “severe” to “mild” or “moderate” to “none,” both of which represent very impactful improvements.
Each subject who reported severe static wrinkles, dynamic wrinkles, surface roughness, scars, visible pores or vasculature at baseline reported at least “mild” severity for these domains at study completion. Moreover, all subjects with “severe” dehydration reported “none” at the end of the study. The blinded reviewer correctly ordered before and after images for 80% of the subjects.
Satisfaction and functional outcomes assessed using subject questionnaires completed on days 21 and 42 revealed that at day 42, 90% of subjects either agreed (50%) or strongly agreed (40%) that they experienced visible reduction of facial fine lines and wrinkles (Figure 4). Overall, 100% of subjects felt that CR-Topical made them more confident in the physical appearance of their face. In agreement with GRS outcomes, subjects strongly agreed that the use of CR-Topical significantly improved the texture/smoothness (90%) and pore size (70%) of the skin, outcomes consistent with those measured with the GRS. Subjects either agreed or strongly agreed (30% vs 70%, respectively) with the statement that they experienced minimal irritation for the duration of the study, demonstrating the excellent tolerability of CR-Topical. Furthermore, 90% of subjects strongly agreed that they were very satisfied with the product, with 90% expressing both their willingness to use CR-Topical again and recommend the cream to family and friends.
Representative patient images illustrate improvement across a range of GRS domains (Figure 5). Changes in skin quality are apparent in before and after images and show a close-up view of patients so that changes in skin quality can be appreciated.
The Benefits of CBD
This pilot study demonstrated that CR-Topical, a novel formulation of retinol, peptides, and antioxidants combined with water-soluble CBD, increases global skin quality and leads to positive subject functional outcomes. While retinol is correlated to a decrease in the depth of fine lines and wrinkles, it is known to have irritating effects on the skin that can lead to erythema, pruritus, peeling, and redness with long-term use.15 Here, these negative effects appear to be counteracted by CBD, improving the tolerability of the product. It will be important to characterize relative tolerability in a split-face study in the future.Although research on CBD oil as a topical agent is still emerging, supplementary use has been shown to decrease inflammation and improve therapeutic outcomes for severe inflammatory skin diseases, supporting this potential role.16-18 Anecdotally, the improvements observed for the combination of retinol and water-soluble CBD are better than for either product alone, suggesting an additive, or potentially synergistic benefit. Larger controlled studies will need to be carried out in order to understand the relative effects of CR-Topical and retinol, and to define any synergistic activity for the two ingredients. Importantly in these studies, a larger number of patients should be followed for an extended period of time to best understand the impact of treatment.
When considering the potential for synergistic activity, the mechanism of action for both retinol and CBD is informative. Through the combined effects of promoting cell proliferation and reducing oxidative stress, these agents may work synergistically to combat both the extrinsic and intrinsic causes of aging. While the mechanism of action of CBD in the skin has yet to be fully elucidated, its antioxidant and anti-inflammatory activities are well recognized, and can be partially attributed to its activation of Nrf2-target activation genes, including HMOX1, which plays crucial roles in modulating inflammation, apoptosis, and oxidative stress.19
Importantly, CBD-induced activation of HMOX1 expression occurs through a Nrf2-independent mechanism.19 Because retinol suppresses expression of Nrf2-target antioxidative genes, the addition of CBD oil can potentially restore antioxidative effects inhibited by retinol while allowing for retention of skin strengthening properties.8,10,18 This activity of CBD is in addition to independent mechanisms, including modulation of the human endocannabinoid system (ECS), which is linked to anti-aging effects through its role in maintaining skin homeostasis and barrier function, antioxidant and anti-inflammatory activity, as well as optimal sebum production.18-20
For retinol, independent effects are manifested through promoting keratinocyte proliferation, strengthening of the epidermis and increasing collagen (through protection of existing collagen and stimulation of neocollagenesis) in the skin.8,9 Importantly, the combination of CBD and retinol appears to reduce skin irritation often observed with retinol alone. Notably, 100% of subjects who reported “severe” dehydration at baseline reported “none” at the conclusion of the study, indicating that CBD may combat the irritation characteristic of retinol topicals, providing considerable benefit to subject tolerability and indirect improvement in efficacy due to increasing the likelihood of adherence. Importantly, the CBD used in this study is water soluble. Most often, CBD is administered dissolved in oil, commonly coconut oil or medium-chain triglyceride (MCT) oil. The absence of oils in this formulation that could potentially clog pores or otherwise irritate skin is also an important contributor.
While improvement across all 13 domains for all subjects suggests a global effect of CR-Topical, improvements in areas such as sagging or asymmetry may signal some variability in day-to-day perceptions, some level of bias that stems from the investigator and the subject completing the assessment together, or incomplete ability of the subject to differentiate entirely between the contributions of individual domains to overall global improvement. In future studies, placebo control and blinding both the subject and evaluating investigator will shed light on this topic. Additionally, when interpreting results, it is important to consider that the rating scale ranged from 0 to 3. Therefore, seemingly modest changes (e.g., “severe” at 3 to “mild” at 1) do indeed reflect a significant improvement. Because of the granular nature of the GRS scale, it is possible that future studies could also evaluate combination treatment with other products or modalities versus monotherapy, further characterizing the effects of distinct interventions on global outcome when used together.
As skin treatments continue to emerge and become increasingly multi-modal in nature, it is essential to better understand the specific effects that different treatments have on the skin. While historical measurements for skin treatment efficacy have relied on static imagery, this methodology cannot capture the movement of glide planes and facial expressions, and it is how our faces move during communication that most informs perceptions of beauty. Capturing movements of the face with short videos more accurately reflects what is observed in day-to-day life as opposed to static imagery, and provides a real-world context for evaluating the most relevant effects of treatment. This novel and dynamic 4D assessment may prevent overcorrection or unnatural looking results by encouraging consideration of youthful dynamics in expression as well as facial proportion.21 Further, 4D assessment can be used in conjunction with new or existing scales and opens the door for incorporation of new measures rating naturalness of outcomes, projection or correction across multiple facial expressions, apparent confidence, openness, or other characteristics that are not traditionally thought of as study outcomes. Moreover, subjects can use the videos to better evaluate their overall satisfaction and experience by observing their facial movements before and after treatment. Like the GRS, 4D assessment can be used as a tool for patient education, treatment planning, and encouraging pursuit of natural-looking results. The exploratory assessment using 4D dynamic imagery in this study revealed that video documentation and 4D beauty is an important element of a comprehensive efficacy profile for any product or device and paved the way for video and dynamic assessments as measures of treatment effect.
Shortcomings of this study include the small sample size and short duration of follow-up time. A larger cohort and increased length of the study could lead to more robust results, especially if the design includes a control group or is a split-face study. Future studies will compare the efficacy of CR-Topical with retinol alone.
When used in combination, water-soluble CBD and retinol offer significant improvements in skin quality, as well as in static and dynamic lines, with minimal irritation. Synergistic activity of CBD and retinol may explain this high level of efficacy. Additionally, a more granular assessment of aesthetic outcomes is long overdue and should be incorporated into future clinical studies evaluating topical skin treatments. Dynamic, 4D beauty assessment is a newly emerging mode of evaluation that could be fully developed and applied to better capture the effects of treatment.
References
1. Zhang S, Duan E. Fighting against skin aging: the way from bench to bedside. Cell Transplant. 2018;27(5):729-738. doi:10.1177/0963689717725755
2. Dimri GP, Lee X, Basile G, et al. A biomarker that identifies senescent human cells in culture and in aging skin in vivo. Proc Natl Acad Sci U S A. 1995;92(20):9363-9367. doi:10.1073/pnas.92.20.9363
3. Kohl E, Steinbauer J, Landthaler M, Szeimies RM. Skin ageing. J Eur Acad Dermatol Venereol. 2011;25(8):873-884. doi:10.1111/j.1468-3083.2010.03963.x
4. Friedman O. Changes associated with the aging face. Facial Plast Surg Clin North Am. 2005;13(3):371-380. doi:10.1016/j.fsc.2005.04.004
5. Rinnerthaler M, Bischof J, Streubel MK, et al. Oxidative stress in aging human skin. Biomolecules. 2015;5(2):545-589. doi:10.3390/biom5020545
6. Tsuchida K, Kobayashi M. Oxidative stress in human facial skin observed by ultraweak photon emission imaging and its correlation with biophysical properties of skin. Sci Rep. 2020;10(1):9626. doi:10.1038/s41598-020-66723-1
7. Mukherjee S, Date A, Patravale V, et al. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging. 2006;1(4):327-348. doi:10.2147/ciia.2006.1.4.327
8. Zasada M, Budzisz E. Retinoids: active molecules influencing skin structure formation in cosmetic and dermatological treatments. Postepy Dermatol Alergol. 2019;36(4):392-397. doi:10.5114/ada.2019.87443
9. Hubbard BA, Unger JG, Rohrich RJ. Reversal of skin aging with topical retinoids. Plast Reconstr Surg. 2014;133(4):481e-490e. doi:10.1097/PRS.0000000000000043
10. Wang H, Liu K, Geng M, et al. RXRα inhibits the NRF2-ARE signaling pathway through a direct interaction with the Neh7 domain of NRF2. Cancer Res. 2013;73(10):3097-3108. doi:10.1158/0008-5472.CAN-12-3386
11. Klassen AF, Cano SJ, Schwitzer JA, Scott AM, Pusic AL. FACE-Q scales for health-related quality of life, early life impact, satisfaction with outcomes, and decision to have treatment: development and validation. Plast Reconstr Surg. 2015;135(2):375-386. doi:10.1097/PRS.0000000000000895
12. Narins RS, Brandt F, Leyden J, Lorenc ZP, Rubin M, Smith S. A randomized, double-blind, multicenter comparison of the efficacy and tolerability of Restylane versus Zyplast for the correction of nasolabial folds. Dermatol Surg. 2003;29(6):588-595. doi:10.1046/j.1524-4725.2003.29150.x
13. Jain R, Huang P, Ferraz RM. A new tool to improve delivery of patient-engaged care and satisfaction in facial treatments: the Aesthetic Global Ranking Scale. J Cosmet Dermatol. 2017;16(1):132-143. doi:10.1111/jocd.12297
14. Cartier H, Hedén P, Delmar H, et al. Repeated full-face aesthetic combination treatment with abobotulinumtoxinA, hyaluronic acid filler, and skin-boosting hyaluronic acid after monotherapy with abobotulinumtoxinA or hyaluronic acid filler. Dermatol Surg. 2020;46(4):475-482. doi:10.1097/DSS.0000000000002165
15. Kim BH, Lee YS, Kang KS. The mechanism of retinol-induced irritation and its application to anti-irritant development. Toxicol Lett. 2003;146(1):65-73. doi:10.1016/j.toxlet.2003.09.001
16. Sholler DJ, Schoene L, Spindle TR. Therapeutic efficacy of cannabidiol (CBD): a review of the evidence from clinical trials and human laboratory studies. Curr Addict Rep. 2020;7(3):405-412. doi:10.1007/s40429-020-00326-8
17. Palmieri B, Laurino C, Vadalà M. A therapeutic effect of cbd-enriched ointment in inflammatory skin diseases and cutaneous scars. Clin Ter. 2019;170(2):e93-e99. doi:10.7417/CT.2019.2116
18. Oláh A, Tóth BI, Borbíró I, et al. Cannabidiol exerts sebostatic and antiinflammatory effects on human sebocytes. J Clin Invest. 2014;124(9):3713-3724. doi:10.1172/JCI64628
19. Casares L, García V, Garrido-Rodríguez M, et al. Cannabidiol induces antioxidant pathways in keratinocytes by targeting BACH1. Redox Biol. 2020;28:101321. doi:10.1016/j.redox.2019.101321
20. Baswan SM, Klosner AE, Glynn K, et al. Therapeutic potential of cannabidiol (CBD) for skin health and disorders. Clin Cosmet Investig Dermatol. 2020;13:927-942. doi:10.2147/CCID.S286411
21. Few JW, Pintas S, Smith JR, Vachon G. Nonsurgical Tissue Repositioning: Analysis of Long-Term Results and Patient Satisfaction From 100 Absorbable Suture Suspension Cases. Aesthet Surg J Open Forum. 2019;2(1):ojz029. doi:10.1093/asjof/ojz029
